Anne R. Crecelius, Associate Professor of Health and Sport Science, University of Dayton
Posted:
Updated:
Your heart beats around 100,000 times every day. Heart rate is a key marker of cardiovascular activity and an important vital sign. But your pulse is not as steady as a precision clock – nor would you want it to be.
As a cardiovascular physiologist, I measure heart rate in nearly every experiment my students and I perform. Sometimes we use an electrocardiogram, such as you’d see in a medical clinic, which uses sticky electrodes to measure electrical signals between two points of your body. Other times we use a chest strap monitor, like ones you might see on someone at the gym, which also detects heartbeats based on electrical activity.
As wearable technology has grown more popular, it’s not just researchers and cardiologists who are paying attention to heart rate. You might be monitoring your own all day long via a fitness tracker you wear on your wrist. This kind of wearable device uses green light to detect blood flow beneath your skin and deduces your heart rate.
Here are what heart rate and other measurements derived from this biometric can tell you about your body’s health.
The heart’s primary job is to contract and generate pressure that helps pump blood to the lungs to be oxygenated and then on to the rest of the body to deliver oxygen and other nutrients. Heart rate is simply how fast your heart is beating. Sometimes called a pulse rate, it’s normally presented in beats per minute. You can count your own heart rate by feeling for your pulse inside your wrist or behind your jaw.
When your body demands more oxygen, such as during exercise, heart rate will increase along with the increasing workloads.
While many people are familiar with tracking their heart rate during exertion, the heart rate at rest can also provide valuable information. The two parts of the autonomic nervous system, the sympathetic and parasympathetic, influence resting heart rate. The sympathetic branch helps coordinate your body’s stress response. The more active it is, the higher it dials up your heart rate, preparing you for fight or flight.
The parasympathetic branch of your nervous system is responsible for keeping lots of your body’s functions running smoothly while you’re at ease. Via the vagus nerve that runs from the brain all the way to the abdomen, the parasympathetic nervous system actively slows the heart down to resting values between 60 and 100 beats per minute for the average healthy adult. Without any parasympathetic activity putting the brakes on the sympathetic nervous system’s signals, your heart would beat at approximately 100 beats per minute.
A lower resting heart rate indicates an efficient heart and a higher level of parasympathetic activity. When you’re at rest your nervous system is ideally minimizing sympathetic activity, so you’re conserving energy and avoiding unnecessary stress to the body.
The chart of a heart rate reveals tiny differences in spacing between the peaks representing heartbeats.YitzhakNat via Wikimedia Commons, CC BY-SA
Time between each heartbeat
One specific way to understand the balance of the nervous system’s influence on heart rate is to look at heart rate variability, or HRV – the slight fluctuation in the time between each heartbeat. Even if your heart rate is 60 beats a minute, that doesn’t mean your heart is pumping exactly once every second.
Less variability is a sign that your body is under greater stress and that the balance in your autonomic nervous system is tipping toward the sympathetic branch being in charge. Greater variability suggests you’re more relaxed and your parasympathetic nervous system is in control.
For nearly 30 years, scientists have been interested in how to measure and interpret HRV, specifically as it relates to this balance of autonomic control.
The clinical utility of HRV emerged in patients following cardiac events, but researchers are now considering how this measure can help explain patient outcomes in a range of cardiac, endocrine and psychiatric disorders.
Researchers have started checking which commercially available wearable devices are most reliable and accurate at measuring HRV, which can vary from tracker to tracker. Many of these devices use colored lights, or optical sensors, to measure pulse rate and other variables at the wrist or finger. Unfortunately, the accuracy of this method can vary based on skin type and skin color. It is important that companies include diverse populations in the design, testing and validation of these products to help address potential racial health disparities.
One of the biggest influences on heart rate variability is stress; along with increased sympathetic nervous system activity, stress is associated with lower HRV. Stress-reducing interventions, biofeedback and increased fitness can increase heart rate variability. Remember, an increase is good for this metric. Overall, heart rate variability depends on a range of physiological, psychological, environmental, lifestyle and nonmodifiable genetic factors.
The most useful way to consider heart rate variability as a metric is to look at data trends. Are there consistent changes in HRV in either direction? Examine these changes alongside other health factors such as fitness, mood, illness, sleep and dietary intake to see if you can draw any conclusions about lifestyle modifications you may want to make.
In general, the same approaches you would take to lowering resting heart rate can also improve heart rate variability, such as increasing cardiovascular fitness, maintaining a healthy weight, reducing stress and getting sufficient sleep.
It’s important to remember that heart rate variability is the normal, healthy, very slight fluctuation of timing of heartbeats – just milliseconds of difference from beat to beat. More dramatic changes in heart rhythms or the way in which the heart contracts, known as arrhythmias, may signal a more serious condition that requires medical attention.
___
Anne R. Crecelius does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
___
PanuShot // Shutterstock
When done correctly, cardiopulmonary resuscitation, or CPR, has the potential to save lives. This technique is used in medical emergencies such as cardiac arrest to maintain the flow of oxygen-rich blood to the brain and throughout the rest of the body. CPR is often performed leading up to emergency medical services’ arrival and until a normal heart rhythm is restored.
For patients who go into cardiac arrest outside of a hospital, there are several factors that increase their chances of making it to the hospital and recovering well enough to be safely discharged. These factors include having the event witnessed by a bystander or emergency medical services and receiving CPR as soon as possible. Researchers have found that survival rates have increased over the last 40 years among those who received CPR up to one year following an out-of-hospital cardiac arrest.
Citing research analyzing CPR survival rate data collected across 88 studies from around the world, ACLS Medical Training looked at how three key factors impact survival rates. These three factors are then broken down into how they impact survival to hospital admission, after discharge from the hospital, and then one month and one year afterward.
PanuShot // Shutterstock
When done correctly, cardiopulmonary resuscitation, or CPR, has the potential to save lives. This technique is used in medical emergencies such as cardiac arrest to maintain the flow of oxygen-rich blood to the brain and throughout the rest of the body. CPR is often performed leading up to emergency medical services’ arrival and until a normal heart rhythm is restored.
For patients who go into cardiac arrest outside of a hospital, there are several factors that increase their chances of making it to the hospital and recovering well enough to be safely discharged. These factors include having the event witnessed by a bystander or emergency medical services and receiving CPR as soon as possible. Researchers have found that survival rates have increased over the last 40 years among those who received CPR up to one year following an out-of-hospital cardiac arrest.
Citing research analyzing CPR survival rate data collected across 88 studies from around the world, ACLS Medical Training looked at how three key factors impact survival rates. These three factors are then broken down into how they impact survival to hospital admission, after discharge from the hospital, and then one month and one year afterward.
Rawpixel.com // Shutterstock
– Survival to admission:
— Bystander CPR: 26.3%
— EMS CPR: 36.3%
— Unspecific CPR: 29.6%
– Survival to discharge:
— Bystander CPR: 22.8%
— EMS CPR: 25.5%
— Unspecific CPR: 21.1%
– One-month survival:
— Bystander CPR: 11.3%
— EMS CPR: 10.7%
— Unspecific CPR: 7.7%
– One-year survival:
— Bystander CPR: 12.8%
— EMS CPR: 12.3%
— Unspecific CPR: 7.9%
When someone’s heart can’t circulate blood on its own, performing CPR can be critical until the patient gets to the hospital. Emergency medical service responders are trained to perform CPR at a rate of 30 compressions per two rescue breaths. EMS responders are essentially acting in place of the heart—each compression manually pushes blood through to the brain and other tissues. Even partially restoring blood flow can increase the chances of resuscitation.
Though bystander CPR has a lower survival rate than EMS responders, it can still improve the chances of survival. The American Heart Association encourages adults and even children to learn hands-only CPR, which is performing 100 to 120 chest compressions per minute with no mouth-to-mouth breaths. Research has found that higher quality CPR training and initiating CPR as soon as possible after a collapse significantly improve long-term survival outcomes.
Rawpixel.com // Shutterstock
– Survival to admission:
— Bystander CPR: 26.3%
— EMS CPR: 36.3%
— Unspecific CPR: 29.6%
– Survival to discharge:
— Bystander CPR: 22.8%
— EMS CPR: 25.5%
— Unspecific CPR: 21.1%
– One-month survival:
— Bystander CPR: 11.3%
— EMS CPR: 10.7%
— Unspecific CPR: 7.7%
– One-year survival:
— Bystander CPR: 12.8%
— EMS CPR: 12.3%
— Unspecific CPR: 7.9%
When someone’s heart can’t circulate blood on its own, performing CPR can be critical until the patient gets to the hospital. Emergency medical service responders are trained to perform CPR at a rate of 30 compressions per two rescue breaths. EMS responders are essentially acting in place of the heart—each compression manually pushes blood through to the brain and other tissues. Even partially restoring blood flow can increase the chances of resuscitation.
Though bystander CPR has a lower survival rate than EMS responders, it can still improve the chances of survival. The American Heart Association encourages adults and even children to learn hands-only CPR, which is performing 100 to 120 chest compressions per minute with no mouth-to-mouth breaths. Research has found that higher quality CPR training and initiating CPR as soon as possible after a collapse significantly improve long-term survival outcomes.
islandboy_stocker // Shutterstock
– Survival to admission:
— Witnessed: 36.4%
— Not witnessed: 36.6%
— Mixed: 23.7%
— Unspecific events: 28.2%
– Survival to discharge:
— Witnessed: 23.2%
— Not witnessed: 24.7%
— Mixed: 21.6%
— Unspecific events: 19.2%
– One-month survival:
— Witnessed: 10.5%
— Not witnessed: 4.4%
— Mixed: 8.2%
— Unspecific events: 8.9%
– One-year survival:
— Witnessed: 13.2%
— Not witnessed: not applicable
— Mixed: 8.3%
— Unspecific events: not applicable
In a randomized clinical trial of 874 patients, those whose cardiac arrest was witnessed by a bystander had more than twice the rate of survival than those whose cardiac arrest was not—but with some caveats.
Although bystanders performed CPR on 32% of patients, early bystander CPR was not associated with increased survival. The researchers found that early bystander CPR didn’t always improve survival either because CPR was not performed properly or its effectiveness decreased after a few minutes. These findings emphasize the importance of raising public awareness about CPR training and early notification of paramedics by bystanders.
islandboy_stocker // Shutterstock
– Survival to admission:
— Witnessed: 36.4%
— Not witnessed: 36.6%
— Mixed: 23.7%
— Unspecific events: 28.2%
– Survival to discharge:
— Witnessed: 23.2%
— Not witnessed: 24.7%
— Mixed: 21.6%
— Unspecific events: 19.2%
– One-month survival:
— Witnessed: 10.5%
— Not witnessed: 4.4%
— Mixed: 8.2%
— Unspecific events: 8.9%
– One-year survival:
— Witnessed: 13.2%
— Not witnessed: not applicable
— Mixed: 8.3%
— Unspecific events: not applicable
In a randomized clinical trial of 874 patients, those whose cardiac arrest was witnessed by a bystander had more than twice the rate of survival than those whose cardiac arrest was not—but with some caveats.
Although bystanders performed CPR on 32% of patients, early bystander CPR was not associated with increased survival. The researchers found that early bystander CPR didn’t always improve survival either because CPR was not performed properly or its effectiveness decreased after a few minutes. These findings emphasize the importance of raising public awareness about CPR training and early notification of paramedics by bystanders.
Miriam Doerr Martin Frommherz // Shutterstock
– Survival to admission:
— Oceania: 33.5%
— Europe: 25.7%
— North America: 20.5%
— Asia: 15.6%
– Survival to discharge:
— Oceania: 16.2%
— Europe: 11.7%
— North America: 7.7%
— Asia: 4.5%
– One-month survival:
— Oceania: 16.0%
— Europe: 9.0%
— North America: 6.5%
— Asia: 12.8%
– One-year survival:
— Oceania: 11.5%
— Europe: 9.2%
— North America: 4.0%
— Asia: 5.3%
Comparing post-CPR survival rates in Europe, North America, Asia, and Oceania (a region that includes Australia and Polynesia), researchers found that there is a higher rate of survival in Western countries. The popularity of CPR classes among the general public is more recent in most Asian countries than in Europe and the U.S., so the quality of bystander CPR may be lower there. South Korea and China have a much higher prevalence of CPR training than other Asian countries, thus survival rates may be higher there.
The threshold for starting CPR by paramedics is also lower in some non-Western countries. These factors may lead to lower survival rates for out-of-hospital cardiac arrest in Asia. Promoting awareness about the importance of CPR training is something governments and health authorities can do to improve outcomes for patients who have out-of-hospital cardiac arrests.
This story originally appeared on ACLS Medical Training and was produced and distributed in partnership with Stacker Studio.
Miriam Doerr Martin Frommherz // Shutterstock
– Survival to admission:
— Oceania: 33.5%
— Europe: 25.7%
— North America: 20.5%
— Asia: 15.6%
– Survival to discharge:
— Oceania: 16.2%
— Europe: 11.7%
— North America: 7.7%
— Asia: 4.5%
– One-month survival:
— Oceania: 16.0%
— Europe: 9.0%
— North America: 6.5%
— Asia: 12.8%
– One-year survival:
— Oceania: 11.5%
— Europe: 9.2%
— North America: 4.0%
— Asia: 5.3%
Comparing post-CPR survival rates in Europe, North America, Asia, and Oceania (a region that includes Australia and Polynesia), researchers found that there is a higher rate of survival in Western countries. The popularity of CPR classes among the general public is more recent in most Asian countries than in Europe and the U.S., so the quality of bystander CPR may be lower there. South Korea and China have a much higher prevalence of CPR training than other Asian countries, thus survival rates may be higher there.
The threshold for starting CPR by paramedics is also lower in some non-Western countries. These factors may lead to lower survival rates for out-of-hospital cardiac arrest in Asia. Promoting awareness about the importance of CPR training is something governments and health authorities can do to improve outcomes for patients who have out-of-hospital cardiac arrests.
This story originally appeared on ACLS Medical Training and was produced and distributed in partnership with Stacker Studio.
totojang1977 // Shutterstock
A surprising number of factors make heart disease the leading cause of death in the United States. Yes, bad habits like smoking and routinely eating an unhealthy diet can lead to heart disease—but so can simply living longer.
Throughout the first half of the 20th century, doctors and scientists developed drugs and treatments for many diseases that once killed people younger, such as tuberculosis and pneumonia. And as people came to live longer, they simply had more time to develop the plaque in their arteries that leads to heart disease.
Although more than 75% of deaths from heart disease occur in low- and middle-income nations, America ranks #2 for deaths from heart disease among 17 peer countries. Public health campaigns across the country have aimed to educate Americans on the causes of heart disease, such as tobacco use, lack of exercise, and eating lots of foods high in cholesterol, while aiming to educate them on how to create habits for better heart health.
Citing 2020 and historical data from the CDC, ACLS Medical Training, a certification company for advanced cardiac life support training, compiled the death rates for heart disease across every state in the U.S., per 100,000 residents. ACLS also provided the mortality rates for three of the most common types of heart disease in the U.S.
totojang1977 // Shutterstock
A surprising number of factors make heart disease the leading cause of death in the United States. Yes, bad habits like smoking and routinely eating an unhealthy diet can lead to heart disease—but so can simply living longer.
Throughout the first half of the 20th century, doctors and scientists developed drugs and treatments for many diseases that once killed people younger, such as tuberculosis and pneumonia. And as people came to live longer, they simply had more time to develop the plaque in their arteries that leads to heart disease.
Although more than 75% of deaths from heart disease occur in low- and middle-income nations, America ranks #2 for deaths from heart disease among 17 peer countries. Public health campaigns across the country have aimed to educate Americans on the causes of heart disease, such as tobacco use, lack of exercise, and eating lots of foods high in cholesterol, while aiming to educate them on how to create habits for better heart health.
Citing 2020 and historical data from the CDC, ACLS Medical Training, a certification company for advanced cardiac life support training, compiled the death rates for heart disease across every state in the U.S., per 100,000 residents. ACLS also provided the mortality rates for three of the most common types of heart disease in the U.S.
Matt Gush // Shutterstock
– Mortality rate per 100k, 2020: 118.1 (8,562 people, +8.0% increase since 2005)

 An increase in this particular biometric is a good thing. visualspace/E+ via Getty Images
An increase in this particular biometric is a good thing. visualspace/E+ via Getty Images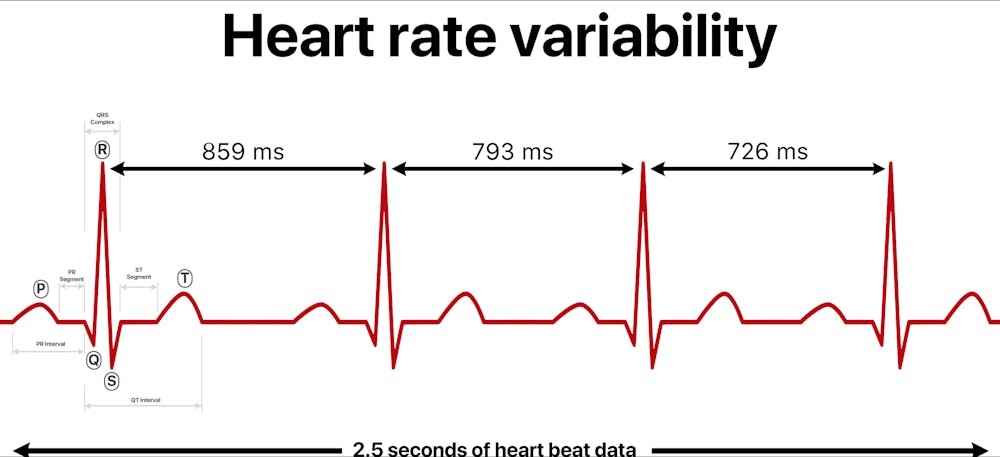 The chart of a heart rate reveals tiny differences in spacing between the peaks representing heartbeats. YitzhakNat via Wikimedia Commons, CC BY-SA
The chart of a heart rate reveals tiny differences in spacing between the peaks representing heartbeats. YitzhakNat via Wikimedia Commons, CC BY-SA Another health benefit of stress-busting activities can be an increase in heart rate variability. David Espejo/Moment via Getty Images
Another health benefit of stress-busting activities can be an increase in heart rate variability. David Espejo/Moment via Getty Images
